
About two and a half years ago our dad was diagnosed with a cancer of the pleura with multiple metastases. It's a type of cancer, which is very common in patients, who've been exposed to asbestos in their lives. It's also incredibly deadly.
The disease has a five-year survival rate of 5% and a median survival duration of about a year (1, 2). This means most patients die within the first 12-ish months and only one in twenty survives to the five-year mark. Thank God, then, that our dad is not just still alive but actively thriving as he's traveling South America with mum.
All tests done before his departure showed, that he was fully cancer-free, but how did he do it? And what has that got to do with you?
Firstly, our dad did have standard of care surgical and chemotherapeutic intervention. As such we always recommend to use the Mosaic Method as supplemental treatment, not as the primary medical treatment. We are working to get the Mosaic Method into clinical trials, but that will presumably take years, if not decades to accomplish.
At the time of diagnosis, neither we nor our dad knew much about cancer. With what he knows nowadays, he says he wouldn't have wanted to take chemotherapy back then, but bygones are bygones and forever remain bygones. But even back then we quickly began looking into cancer and where the research on the disease is headed.
In so doing we developed the Mosaic Method, consisting of seven primary measures:
- Stop all consumption of carbohydrates
- Eliminate all possible consumption of glutamine and glutamate
- Maximise fat consumption
- Supplement vitamin D3 and omega-3 fatty acids
- Supplement EGCG and curcumin
- Eliminate all oxalates, alcohol, and pro-inflammatory substances
- Keep a positive mind at all times
Dad does these to the full extent for six weeks every year to stop reemergence of cancer and does them to a looser extent during the rest of the year. His focus is on eliminating carbohydrate consumption and maximising fat consumption, though he does supplement vitamin D3 and curcumin. Moreover, he has a low to very low consumption of glutamine, glutamate, oxalates, and pro-inflammatory substances.
If this is enough for you, and you don't want to know the logic behind the Mosaic Method, feel free to stop reading here.
With everyone reading on, let's get into the meat of this article. We want to understand cancer on a basic level and then understand how exactly each of the seven measures of the Mosaic Method above attacks cancer.
We'll start off with a banger: There one central fact about cancer, which oftentimes goes completely overlooked. And that fact is this: There's only one kind of cancer, which can kill us: a growing one. If a cancer doesn't grow, it can't kill us.
You may doubt this, but here's a silly question: Are you alive?
I presume the answer is a stark 'Yes!'. Splendid. That means, you cancer is too small to kill you. If it suddenly stopped growing or even shrunk, you'd outlive it, even if a small part of it remains. Halting cancer growth, protects against death from cancer. Inverting cancer growth, winds back the time on your clock.
There are thus two ways in which we can outlive cancer:
- By lowering cancer cell growth rate.
- By increasing cancer cell death rate.
That's it. It's that 'simple'. Though that far from makes it easy. It is possible, but incredibly difficult. There's nothing, that will take away your fear, your uncertainty, your pain, your sacrifice in dealing with a disease as vicious as cancer. Let me be very clear on that. Just as there are no promises. Outliving cancer has been done and it can generally be done, but with as much as we do know about cancer, when it comes to biology, we – humanity – are still children. There's always something we don't know, always something new to learn.
Still, I trust that this will prolong your life and improve your quality of life all the same.
But how can I say these things, when modern medicine has failed so horrendously at the task of defeating cancer, even after decades of research and billions of USD spent?
We publish new articles, whenever we've synthesised new findings to a usable degree. You can subscribe to receive articles for free.
There's a central problem with all these decades of research. They overlook a quite critical fact about cancer: the primary cause of cancer is NOT somatic mutation, but metabolic degeneracy. Big words, but what do they mean, and most importantly, what's this got to do with you?
There have been two competing theories in the explanation of the origin of cancer as a disease. These two theories are the 'somatic mutation theory' on one side and the 'metabolic theory' on the other. To understand, what these theories posit, we first need to take a look at basic cellular anatomy.
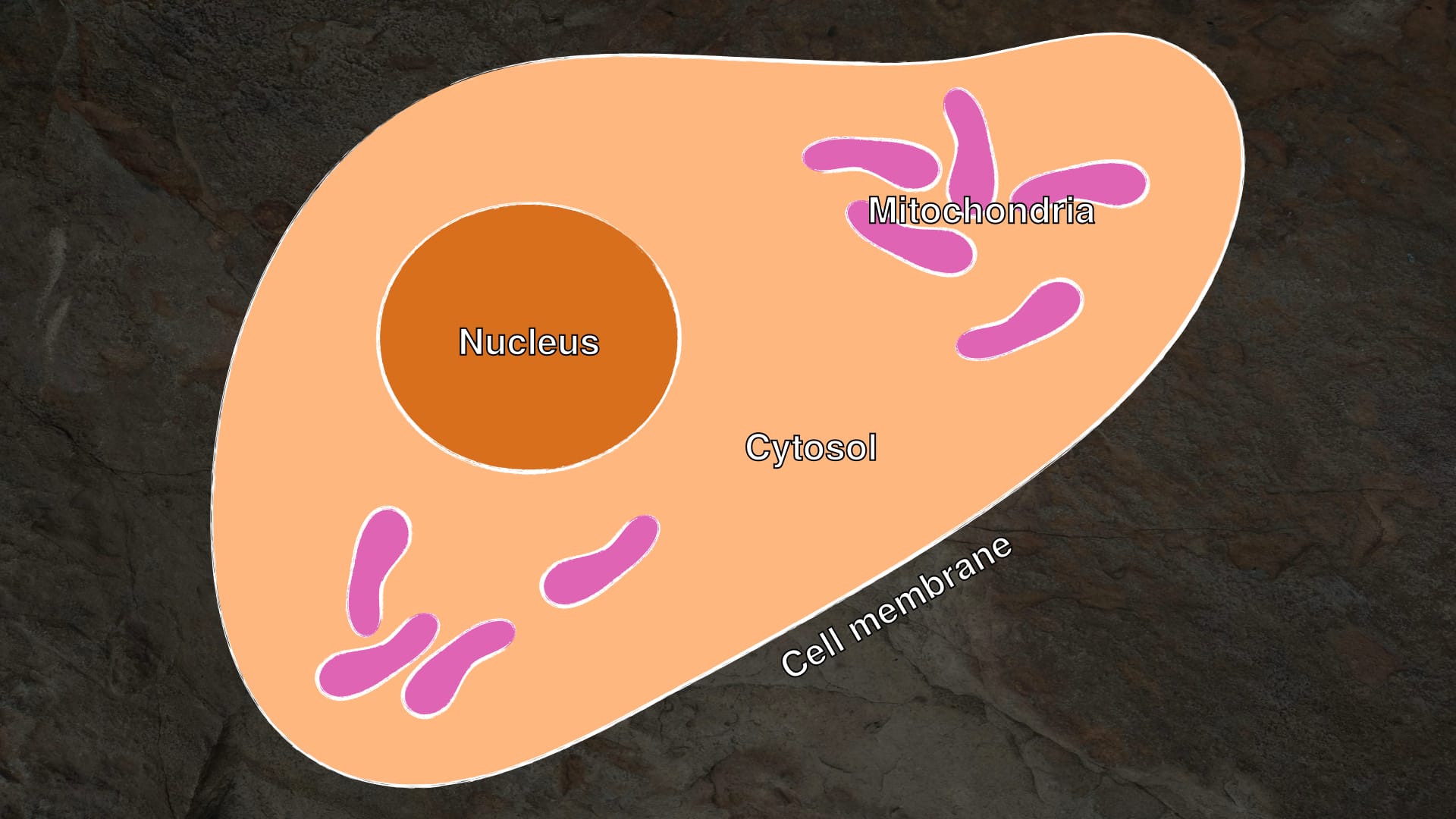
A cell is characterised by having biological machinery surrounded by a cell membrane (Fig. 1 – 1). This biological machinery is suspended in water and known collectively as 'the cytosol' (Fig. 1 – 2), which is where the bulk of a cell's metabolism is located. Our normal energy metabolism, specifically, is located within a structure of the cytosol called the mitochondria (Fig. 1 – 3). This is where aerobic energy production takes place. Aerobic energy production uses oxygen, whereas anaerobic energy production – aka. fermentation – doesn't. This will become important later, but I wanted to give you the overview here.
Within nucleated cells – such as our mammalian cells – there's another big structure, which is easily differentiated from the rest of the cytosol. This feature is the cell nucleus (Fig. 1 – 5), which holds the cell's genome and is segregated from the rest of the cell's interior by the nuclear envelope (Fig. 1 – 4).
The somatic mutation theory states, that cancer is primarily caused by mutation in the nuclear genome of cells, which then changes the cell behaviour from that of a healthy cell to that of a cancerous cell.
The metabolic theory states, that cancer is primarily caused by degeneracies in cell metabolism, which destabilise the genome and thus both directly and indirectly changes the behaviour of the cell.
But how can we know which one is true? Or at least, which one of these is closer to the truth? I'm aware of two interesting experiments, which give us an indication.
In the first experiment, I have in mind, healthy cells were cultured alongside cancerous cells. Healthy cells hereby have both normal cytosol and nuclear genome, whilst the cancerous cells have both abnormal cytosol and nuclear genome. With these pre-cultured cells researchers performed to actions: they transferred a cancerous nucleus into a healthy cytosol and vice versa they transferred a healthy nucleus into a cancerous cytosol (Fig. 2 – left and right) (3).
Now, let's pause and consider the two competing theories of cancer and what results they would predict of this experiment.
The somatic mutation theory posits, that the cause of cancer is genetic. As the nucleus holds the genome of a cell, transfer of the nucleus from a cancerous cell to a cell with a healthy cytosol should give rise to a cancerous cell, regardless of the cytosol. Thus, the somatic mutation theory predicts, that the cancerous cytosol–healthy nucleus hybrid would become a healthy cell with normal metabolism and growth regulation, whereas the healthy cytosol–cancerous nucleus hybrid would become a cancerous cell, with degenerate metabolism and growth regulation.
The metabolic theory posits, that the cause of cancer is metabolic. As the cytosol holds the metabolism of a cell, the cytosol of a cancerous cell should give rise to a cancerous cell, regardless of the nucleus transplanted into it. Thus, the metabolic theory predicts, that the cancerous cytosol–healthy nucleus hybrid would become a cancerous cell – despite the healthy nucleus –, and that the the healthy cytosol–cancerous nucleus hybrid would become a healthy cell – in spite of the cancerous nucleus.
To summarise: the somatic mutation theory tells us 'healthy nucleus, healthy cell', and the metabolic theory tells us 'healthy cytosol, healthy cell'.
So, what did the experiment show?
It showed the latter. The experiment showed, that a cancerous nucleus, when transplanted into a healthy cytosol gives us a healthy cell (Fig. 2 – left), whereas a healthy nucleus, when transplanted into a cancerous cytosol gives us a cancerous cell (Fig. 2 – right). Thus, what seems to be the primary metric of concern is the health of the cytosol, not so the health of the nucleus.
Interesting, but it gets better in the next experiment.
It's well known, that cancer cells often lose a feature called 'differentiation'. 'Differentiation' is just a fancy word to describe a cell's specialisation in the broader scope of our body's function. Every cell in our body, which takes up a specific function in a tissue, organ, or system is differentiated. Liver cells, lung cells, immune cells, and nerve cells are so different from one another and fulfil so vastly different roles, because they have gone through the process of differentiation, and thus specialise in a highly specific function or set of functions.
Cancers often derive from these specialised cells or their precursors, but they often times lose their differentiation – i. e. they stop fulfilling their function as a part of our body and become defective.
Now, whilst there seems to be some merit to this, the abnormalities of the nuclear genome don't seem to be solely responsible for loss of differentiation. This is something the second experiment I had in mind shows very nicely with a type of frog tumour (4).
In the given experiment, the nucleus of a cancerous cell was transplanted into a healthy and activated oocyte (colloquially 'egg cell'). Following somatic mutation theory, this cancerous cell nucleus with its defective genome should not be able to generate any kind of differentiated cells, never mind a fully differentiated complex organism.
We don't take sponsoring or display advertisements in order to keep us free from conflicts of interest. If you've found this valuable, you can help us by supporting our fight against cancer financially.
This is, however, precisely what happened. Some of the hybrid cells of cancerous nucleus and healthy oocyte went through normative differentiation all the way into the tadpole stage. In this tadpole stage, those that survived thus far, were responsive to stimulus and able to swim without issue. They had a functioning nervous system, circular system, and were even able to regenerate parts of their tail, when clipped. The latter is normal in tadpoles. This means, that the cancerous nucleus was able to differentiate into all necessary cell types of the tadpole. Genetic degeneracy thus cannot be the singular reason for loss of differentiation of such cancer cells.
What does this show us for cancer, though? And what does this mean for us?
Well, this shows us that accepting somatic mutation – meaning the mutation of the nuclear genome of differentiated cells – as the primary cause of cancer is nonsensical and not supported by the evidence.
Cancer much rather seems to be a disease caused by degenerate cytosol, and thereby degenerate metabolism. Mind you, this doesn't mean, that genetic degeneracy plays no role. Genetic degeneracy and loss of differentiation clearly plays a role in the potential of cancer to cause damage and fatality in a patient, but the root cause remains the degenerate cytosol.
Our primary effort should thus be to normalise cytosolic function throughout our entire body, but especially in cancer cells. This is precisely the result the above seven measures against cancer aim at.
But... I promised you to explain cancer deeply enough for you to understand each of the seven measures and their impact upon cancer growth and death rates – and thereby cancer-caused mortality.
So, let's take a look at the attributes, which differentiate cancerous cells from normal cells.
One of the most prominent of these attribute is the 'Warburg effect', which has been known since the 1920s and hasn't been used as an attack point for treatment en masse. The Warburg effect describes the tendency of cancer cells to rely on oxygen-less energy production, even when oxygen is plentiful.
Now, what does that mean?
Oxygen-dependent energy production is the main avenue of energy production within our cells, simply because it's the most efficient mode of energy production when considering the energy output per mass of fuel (6). This oxygen-dependent energy production is performed in our mitochondria via a process known as 'cellular respiration' (7). Cellular respiration is comprised of multiple component processes, but for simplicity, I'll only refer to cellular respiration collectively.
Our cells do, however, have a much older and far less efficient avenue of energy production available to them. This less efficient mode of energy production is 'cellular fermentation' and normally only happens, when oxygen is unavailable (5).
This is where cancerous cells differ. They will use fermentation, even when oxygen is available and plentiful.
Cancer cells do this, because their mitochondria are damaged and no longer function properly and thus can't supply the cell with energy anymore (8). The cancerous cell will then rely on fermentation, no matter the availability of oxygen. This has some catastrophic effects.
Firstly, mitochondria are one of the primary 'quality control units' in our cells, and beside energy production, they are also responsible for initiating a cellular suicide in the event, that a cell becomes too damaged or dangerous to the organism as a whole. By losing function of their mitochondria, cancer cells gain a resistance to this crucial protection mechanism. They no longer die, when they become too damaged or dangerous for our body (9).
Secondly, by activating the ancient energy production pathway of fermentation, cancer cells begin to revert to a behaviour far older than complex multicellular life. This means, that our cancer cells transition from acting as constituent parts of a multicellular organism – which we humans are – to acting as a colony of single-celled organisms, much like bacteria (10). This is the effect of the loss of differentiation discussed above. And much like bacteria, the cancer cells will begin to divide rapidly and quickly grow out of control.
Thirdly, by reverting to an older behaviour, supportive of single-celled life, cancerous cells begin to acquire mobility and invasive capabilities. Most of our cells are exceedingly stationary and their spacial positioning tightly controlled. Cancerous cells, by virtue of their loss of differentiation, will begin to overstep their bounds and invade foreign tissues or even enter the blood stream and relocate to an entirely different site within our body (11). The former is called invasion, the latter is called metastasis.
You may now understand intimately, why it's crucial to rehabilitate mitochondria in cancerous cells and force cancerous cells away from a fermentation-based metabolism.
And this is where we'll now be able to understand some of the logic behind the seven measures above.
We want to stop cancerous cells from using fermentation. We can do this in two ways. Either we restrict the availability of fermentable fuels, or we biochemically inhibit those pathways cancer cells use for fermentation.
There are two fuels, which cancer cells can ferment: glucose and glutamine (10).
So, by eliminating all carbohydrates (and sugar) from our diet, we can lower the availability of glucose. This is measure 1 of our Mosaic Method above. This is most easily done by fully abstaining from plant products, all non-cheese, non-butter dairy, as well as honey. Some plant products, which are fine with regard to carbohydrate consumption, will be problematic to other measures of the Mosaic Method. These other measures we will explore in another article.
By lowering all glutamine and glutamate consumption as far as possible – glutamine and glutamate are largely interchangeable –, we can lower the availability of glutamine. This is measure 2 of the Mosaic Method and is most simply done, by abstaining from cereals, which have a high load in glutamate (12).
But there's more to be done on the 'stopping fermentation' front.
We can for example further inhibit glutamine fermentation by supplementation of the compound 'EGCG'. EGCG – or 'epigallocatechin-3-gallate' – is a compound found abundantly in green tea, which inhibits glutamine fermentation, alongside a host of other anti-cancer actions (13). These other actions shall be important in another article, where we'll go into attack points of cancer, which are not directly linked to the metabolic degeneracy of cancer. We can drink green tea for EGCG, but the quantity of consumption is more trackable and measurable in the form of a supplement. The supplementation should hereby not exceed 800 mg per day, because liver-toxicity may occur at 800 mg/day over a duration of 4 months or more (13).
We can also inhibit glutamine fermentation by supplementation of the compound 'curcumin'. Curcumin is a compound found in turmeric. It has been show to decrease cancer cell viability and growth, as well as increase cancer susceptibility to chemotherapy drugs by inhibiting glutamine metabolism (14). Dosing curcumin is a bit difficult, as it's not very bioavailable. This means, that most of the curcumin, which is ingested leaves your digestive tract with your excrement. It's known, however, that dosages of up to 12 g/day of curcumin in oral application are not problematic (15). There are some formulations, which promise better bioavailability, one of which is called novaSOL and is ostensibly based on a study in 'Molecular Nutrition and Food Research' in 2014, which the marketers don't cite directly (probably reference 16, but I'm unsure). The study show's higher bioavailability, so this might be interesting for you, but I'd advice caution with such products. More information is needed. The safety of the oral curcumin, however, seems unaffected by the formulation.
We can also increase systemic pressure away from fermentation and toward an oxygen-dependent metabolism, by maximising fat consumption and thus entering the metabolic state of ketosis, which has shown promise in improving survival in cancer patients and mouse models (17–9). This holds true even with patients (or mouse subjects) with multiple metastases – meaning with highly aggressive cancer, which has spread throughout the body. Ketosis is a metabolic state of fat-utilisation and by maximising dietary fat and eliminating other fuels – carbohydrates and glutamine/glutamate, we can begin to force cancerous cells away from fermentation and back to a normalised metabolism.
By maximising fat consumption, I mean, that your body should only be deriving energy from fat. This can easily be achieved by eating animal products only, whilst excluding non-cheese, non-butter dairy. This should be done with testing of ketosis and optionally breath ammoniac. Ketosis is usually tested for via blood ketone values or breath acetone. Since ketosis is the state of using fat for fuel, remaining in ketosis is crucial. If ketosis is not achieved by eating animal products only under exclusion of non-cheese, non-butter dairy, increasing fat content in diet should help with achieving ketosis. There are devices, which can test for breath ammoniac, but if you have loved ones, that say you've started having a stinky breath, it's probably ammoniac. If breath ammoniac is present, increasing fat content in diet should help with lowering breath ammoniac. If this doesn't help, further lowering dietary protein content may help.
The normalisation of the metabolism thus achieved will to the best of our knowledge normalise mitochondrial function or force cancer cells into death. This is supported in research, where mitochondria induced cancer cell suicide (apoptosis), when the cancer cell was pharmacologically forced to use mitochondrial energy production (20). Now it's important to remember, that it's in the mitochondria, where aerobic energy production takes place, and that fermentation takes place in the cytosol. Thus, the cancer cell was forced to use mitochondrial aerobic energy production in this study by bichloroacetic acid, which is broadly used in humans, but has shown neuropathy and should thus only be used under professional surveillance (21)!
Now this brings us to the conclusion of this article.
So, let's go back to the seven anti-cancer measures of the Mosaic Method:
- Stop all consumption of carbohydrates
- Eliminate all possible consumption of glutamine and glutamate
- Maximise fat consumption
- Supplement vitamin D3 and omega-3 fatty acids
- Supplement EGCG and curcumin
- Eliminate all oxalates, alcohol, and pro-inflammatory substances
- Keep a positive mind at all times
We now understand the logic behind measures 1–3 and 5. We will get to understand the other measures in more depth in a future article, but they are a topic for another time.
This is our Mosaic Method laid bare. I recommend you steal it for your own anti-cancer success. May God bless you and may you outlive cancer.
And again, if you ever need help, you can find resources or direct help from us at www.marchward.com.
References
- Milano, M.T., and Zhang, H. (2010). Malignant Pleural Mesothelioma: A Population-Based Study of Survival. Journal of Thoracic Oncology 5, 1841-1848. 10.1097/JTO.0b013e3181f1cf2b.
- Mazurek, J.M., Syamlal, G., Wood, J.M., Hendricks, S.A., and Weston, A. (2017). Malignant Mesothelioma Mortality - United States, 1999-2015. MMWR Morb Mortal Wkly Rep 66, 214-218. 10.15585/mmwr.mm6608a3.
- Seyfried, T.N., and Chinopoulos, C. (2021). Can the Mitochondrial Metabolic Theory Explain Better the Origin and Management of Cancer than Can the Somatic Mutation Theory? Metabolites 11.
- McKinnell, R.G., Deggins, B.A., and Labat, D.D. (1969). Transplantation of Pluripotential Nuclei from Triploid Frog Tumors. Science 165, 394-396. 10.1126/science.165.3891.394.
- Alfarouk, K.O. (2016). Tumor metabolism, cancer cell transporters, and microenvironmental resistance. Journal of Enzyme Inhibition and Medicinal Chemistry 31, 859-866. 10.3109/14756366.2016.1140753.
- Alberts, B., Johnson, A., Lewis, J., Morgan, D., Raff, M., Roberts, K., and Walter, P. (2015). Cell Chemistry and Bioenergetics. In Molecular Biology of the Cell, (Garland Science, Taylor & Francis Group, LLC), pp. 43-108.
- Alberts, B., Johnson, A., Lewis, J., Morgan, D., Raff, M., Roberts, K., and Walter, P. (2015). Energy Conversion: Mitochondria and Chloroplasts. In Molecular Biology of the Cell, (Garland Science, Taylor & Francis Group, LLC), pp. 753-812.
- Seyfried, T.N., Arismendi-Morillo, G.J., Mukherjee, P., and Chinopoulos, C. (2020). On the Origin of ATP Synthesis in Cancer. iScience 23.
- Seyfried, T.N., and Shelton, L.M. (2010). Cancer as a metabolic disease. Nutrition & Metabolism 7, 7 - 7.
- Alfarouk, K.O., Shayoub, M.E.A., Muddathir, A.K., Elhassan, G.O., and Bashir, A.H.H. (2011). Evolution of Tumor Metabolism might Reflect Carcinogenesis as a Reverse Evolution process (Dismantling of Multicellularity). Cancers 3, 3002-3017.
- Seyfried, T.N., and Huysentruyt, L.C. (2013). On the origin of cancer metastasis. Critical reviews in oncogenesis 18 1-2, 43-73.
- Dai, Z., Zheng, W., and Locasale, J.W. (2022). Amino acid variability, tradeoffs and optimality in human diet. Nature Communications 13, 6683. 10.1038/s41467-022-34486-0.
- Talib, W.H., Awajan, D., Alqudah, A., Alsawwaf, R., Althunibat, R., Abu AlRoos, M., Al Safadi, A.a., Abu Asab, S., Hadi, R.W., and Al Kury, L.T. (2024). Targeting Cancer Hallmarks with Epigallocatechin Gallate (EGCG): Mechanistic Basis and Therapeutic Targets. Molecules 29, 1373.
- Thongpon, P., Intuyod, K., Chomwong, S., Pongking, T., Klungsaeng, S., Muisuk, K., Charoenram, N., Sitthirach, C., Thanan, R., Pinlaor, P., and Pinlaor, S. (2024). Curcumin synergistically enhances the efficacy of gemcitabine against gemcitabine-resistant cholangiocarcinoma via the targeting LAT2/glutamine pathway. Scientific Reports 14, 16059. 10.1038/s41598-024-66945-7.
- Park, W., Amin, A.R., Chen, Z.G., and Shin, D.M. (2013). New perspectives of curcumin in cancer prevention. Cancer Prev Res (Phila) 6, 387-400. 10.1158/1940-6207.Capr-12-0410.
- Schiborr, C., Kocher, A., Behnam, D., Jandasek, J., Toelstede, S., and Frank, J. (2014). The oral bioavailability of curcumin from micronized powder and liquid micelles is significantly increased in healthy humans and differs between sexes. Molecular Nutrition & Food Research 58, 516-527. 10.1002/mnfr.201300724.
- Poff, A.M., Ari, C., Arnold, P., Seyfried, T.N., and D'Agostino, D.P. (2014). Ketone supplementation decreases tumor cell viability and prolongs survival of mice with metastatic cancer. International Journal of Cancer. Journal International du Cancer 135, 1711 - 1720.
- Seyfried, T.N., Flores, R., Poff, A.M., D’Agostino, D.P., and Mukherjee, P. (2015). Metabolic therapy: A new paradigm for managing malignant brain cancer. Cancer Letters 356, 289-300. 10.1016/j.canlet.2014.07.015.
- Weber, D.D., Aminzadeh-Gohari, S., Thapa, M., Redtenbacher, A.-S., Catalano, L., Capelôa, T., Vazeille, T., Emberger, M., Felder, T.K., Feichtinger, R.G., et al. (2022). Ketogenic diets slow melanoma growth in vivo regardless of tumor genetics and metabolic plasticity. Cancer & Metabolism 10, 12. 10.1186/s40170-022-00288-7.
- Bonnet, S., Archer, S.L., Allalunis-Turner, J., Haromy, A., Beaulieu, C., Thompson, R., Lee, C.T., Lopaschuk, G.D., Puttagunta, L., Bonnet, S., et al. (2007). A Mitochondria-K+ Channel Axis Is Suppressed in Cancer and Its Normalization Promotes Apoptosis and Inhibits Cancer Growth. Cancer Cell 11, 37-51. 10.1016/j.ccr.2006.10.020.
- Michelakis, E.D., Webster, L., and Mackey, J.R. (2008). Dichloroacetate (DCA) as a potential metabolic-targeting therapy for cancer. Br J Cancer 99, 989-994. 10.1038/sj.bjc.6604554.






